
The first annual report of statistical information concerning euthanasia (MAID) was released in July by Health Canada. Its data comes from Canada’s federal monitoring and reporting regime which came into effect in November 2018. Previously, the department had compiled and released four interim reports.
This latest report does not address possible abuses of the law. The independent report from Quebec’s Commission des soins de fin de vie dated to October 2019 found that at least 13 euthanasia deaths in the province did not meet legal requirements.
Health Canada says that “with respect to oversight, some jurisdictions such as, Manitoba, Saskatchewan, Alberta, and British Columbia have implemented review committees to ensure MAID is being provided in accordance with federal and provincial rules. In Ontario, all MAID deaths are reported to the Chief Coroner’s office who is also responsible for oversight.”
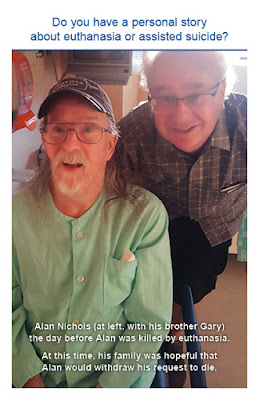
Has the review committee in British Columbia looked into the case of Alan Nichols who died by euthanasia at Chilliwack General Hospital in July 2019? His family members were stunned that Alan was approved for euthanasia. Mr. Nichols had a history of chronic depression but was not sick or dying. His brother and sister were unsuccessful in their efforts to stop his death by euthanasia.
Health Canada calls attention to media reports concerning faith based institutions and palliative care centres who refuse to allow euthanasia assessments or its provision in their facilities. We are told that “This has resulted in patients being required to transfer to another facility if they wish to receive the procedure.” Yet, transfers to another facility for surgeries, procedures or tests are routine matters in health care. Why is it that media reports concerning the coercion of hospices are not mentioned? The Ministry of Health for British Columbia is threatening to pull funding from the Delta Hospice Society because it will not allow euthanasia to take place on its centre’s premises. The Delta Hospice Society continues its legal battle. The Serenity hospice in North Bay is also being coerced by four local physicians who want the hospice to offer euthanasia on site. Health Canada also fails to mention media reports regarding cases of patients with disabilities who experienced pressure in the direction of euthanasia, Roger Foley and Candice Lewis.
Health Canada does provide however favourable anecdotal accounts from practitioners of their patients’ death by euthanasia: “Patient who passed away in her garden, sitting in her favourite chair, surrounded by friends and family. Balloons were released before her death (to help guide her on her journey…) She reportedly told her daughter that she would not have been able to manage another week.” The information provided in Health Canada’s latest report consists of data collected from physicians, nurse practitioners and pharmacists. We know only what the practitioner causing the death, reports to the designated provincial or territorial body or directly to Health Canada.

5,631 ‘assisted deaths’ were reported for 2019. The overwhelming majority (5,624) were euthanasia cases done by lethal injection by a practitioner. There were fewer than 7 cases consisting of assisted suicide where the individual self administers the lethal dose. The total number of euthanasia (MAID) deaths stands at 13,946 in Canada since the federal law was passed in June 2016. The 2019 numbers represent a 26.1% increase over 2018 numbers.
Euthanasia (MAID) deaths represent 2% of all deaths in Canada. In British Columbia, euthanasia deaths are 3.3% of all deaths and in Quebec, 2.4% of all deaths.
Those who are 56 years of age and older account for 93.4% of euthanasia deaths.
The report tells us that there were 1,271 “unique practitioners” providing euthanasia in 2019. 1,196 are physicians and 75 are nurse practitioners. Family physicians make up 65% of those willing to give lethal injections, palliative care medicine specialists (9.1%), and anesthesiologists (5%).
⦁ 617 practitioners (48.5%) provided one euthanasia procedure.
⦁ 528 practitioners (41.5%) provided the procedure 2 to 9 times.
⦁ 126 practitioners (9.9%) provided the procedure more than 10 times during the year.
According to practitioners, loss of autonomy was the primary reason given as cause of suffering by patients.
Loss of ability to engage in meaningful life activities: 82.1%
Loss of ability to perform activities of daily living; 78.1%
Inadequate control of symptoms other than pain (or concern about it): 56.4%
Inadequate control of pain or concern about it: 53.9%
Loss of dignity: 53.3%
Perceived burden on family, friends or caregivers: 34.0%
Loss of control of bodily functions: 31.9%
Isolation or loneliness: 13.7%
7,336 written requests were received in 2019. Of these, 5,389 (73%) resulted in euthanasia.
For 1,947 requests, euthanasia was not administered for the following reasons: in 1,113 cases the patients died before receiving a lethal injection. In 571 cases, the patients were considered ineligible. In 263 cases, the patients withdrew their requests.
For the 7.8% determined to be ineligible for euthanasia, the reasons given were:
⦁ A lack of capacity to make medical decisions: 32.2%f cases.
⦁ The person’s natural death was not reasonably foreseeable: 27.8% of cases
⦁ The person was not considered to be in a state of irreversible decline in capacity: 23.5%of cases.
A physician or nurse practitioner must report all written requests for euthanasia. As well, they must report the age, sex, postal code, assessment of the request, eligibility of the person and whether two practitioners approved the eligibility and whether there was a 10 day reflection period between the time of the request and the actual procedure being done.
In 65.7% of cases, the 10 day requirement was met. In 34.3% of cases, the 10 day reflection period was shortened with 84.4% of practitioners giving “imminent loss of the patient’s capacity to consent as the primary reason, with imminent death cited in 45.4% of these cases.”
For all patients receiving euthanasia, the practitioner must report if the patient received palliative care and or disability supports services if these were needed.
- Cancer was the medical condition most associated with euthanasia at 67.2% of cases.
- Respiratory conditions accounted for 10.8% of euthanasia deaths.
- Neurological conditions followed at10.4% of cases and cardiovascular at 10.1% of cases.
- At 6.1% of cases, a category called Other Condition is described as including “a range of conditions, with frailty commonly cited.”
Administration of euthanasia occurred primarily in hospital or at home. 36.3 % in hospital (excluding palliative care beds) and in the patient’s residence (35.2%). 20.6% took place in a palliative care unit.
Health Canada states that “It should be noted that there is nothing in the federal MAID legislation that compels a practitioner to provide or assist in providing MAID.” We would point out that there is nothing in the federal legislation that provides specific conscience rights protection for physicians, nurses and other health practitioners. In fact, a policy of the Ontario College of Physicians and Surgeons explicitly requires physicians or nurses to make referrals for euthanasia in spite of their conscientious objection to it. Health professionals continue to ask for legislation to provide specific protection.
Source: First Annual Report on Medical Assistance in Dying in Canada 2019. Health Canada, July 2020.



{kind=link}
{kind=link}
{kind=link}